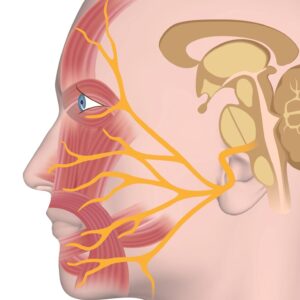
The facial nerve, also called cranial nerve VII, is one of the twelve cranial nerves that come directly from the brain. It starts in the brainstem and travels through the skull to reach the face. Along its path, the nerve branches out into smaller nerves that control different parts of the face. These branches are responsible for moving the muscles of facial expression, like smiling, frowning, or closing the eyes. The facial nerve also carries signals to some glands, such as the salivary and tear glands, and helps with taste on the front two-thirds of the tongue (Standring, 2021). .
The main job of the facial nerve is to control facial movements and expressions, but it also has sensory and secretory functions. It helps us show emotions through our face, taste sweet and salty flavors, and even keep our eyes moist by stimulating tear production. Because the facial nerve has many roles, damage to it can cause weakness or paralysis on one side of the face, loss of taste, or dryness in the eyes and mouth (Brazis, Masdeu, & Biller, 2012).